
By Helen Petousis-Harris
If the risk is as small, as it currently appears to be, then we need to ask ourselves if it is worth using these vaccines and if so, in whom.
What has happened?
Recently the vaccine safety watch dogs in Europe noted reports of unusual types of blood clots in people vaccinated with the AstraZeneca (AZ) COVID-19 vaccine. This prompted investigations across many countries to ascertain what, why, and how. Also, in recent days, the U.S. has reported unusual types of blood clots in people vaccinated with the Janssen/Johnson & Johnson COVID-19 vaccine.
Observations so far suggest that in younger AZ vaccinees, primarily women, there might be an unusual type of blood disorder that involves both low platelets (that can lead to bleeding) and blood clotting at the same time (thrombocytopenia and thrombosis). This disorder is appearing a week or two after vaccine administration and has been named Thrombosis with Thrombocytopenia Syndrome (TTS). It has been likened to a condition associated with the commonly used blood thinning drug, heparin, although the risk with the vaccine is far lower.
What are the risks?
The risk of developing this syndrome after receiving either the AZ or Janssen viral vector vaccines is miniscule. You are truly more likely to be struck by lightning in your lifetime. However, for those who do develop these blood clots the consequences can be dire with ¼ dying, and this is why the condition is being taken very seriously. The higher number of cases appearing in women may be because more women have been vaccinated.
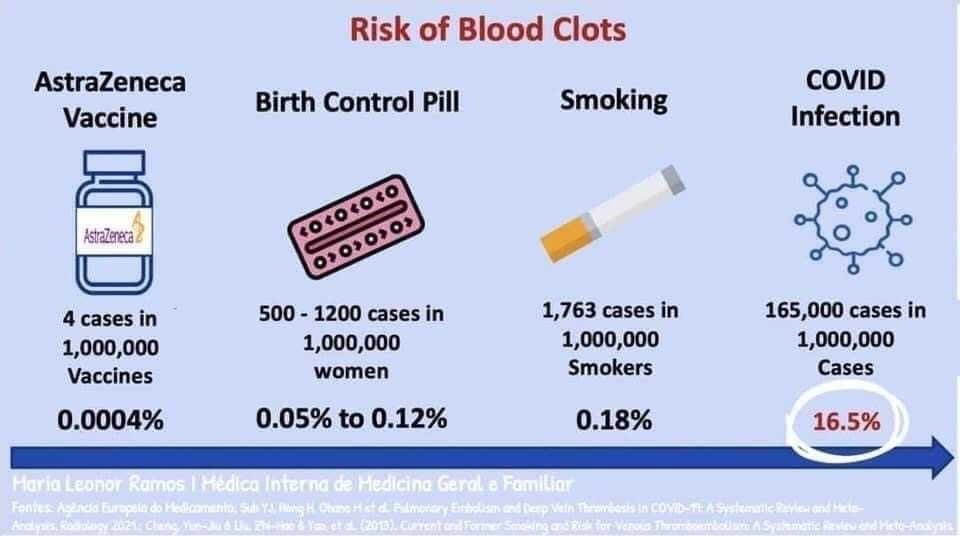
Here are some comparisons:
- AstraZeneca vaccine ~4 per million vaccines
- Janssen viral vector COVID vaccine ~1 per million vaccines
- Pfizer mRNA COVID vaccine no signal >100 million vaccines
- Moderna mRNA COVID vaccine no signal <100 million vaccines
- Birth Control Pill[i] 150-800 per million women
- Smoking 1,700-1,800 per million smokers
- Severe COVID infection ~165,000 per million cases
- Getting struck by lightning this year (US)[ii] 1 per 1.2 million
- Getting struck by lightning in your life (US)[iii] 65 per million
Why are we picking this up now?
We are picking this up now because of the sheer number of people being vaccinated at the same time (~820 million doses globally since December). Big numbers are really the only way very rare side effects can be detected, there is no way a clinical trial can pick these up, they are not big enough. The fact that this has been identified is an indication that the safety monitoring systems are working pretty well. These are the surveillance systems that watch for adverse events after medicines start being used in the population. While some alerts turn out to be false alarms, others turn out to be real.
How will we know if this condition is truly caused by the vaccines?
While we have seen reports of unusual blood clots, this does not mean they are definitely caused by the vaccine. There are two more steps that need to be carried out.
- First, we need to compare what we are observing to what we expect and to do this we need to know how many cases of this condition occur normally in the background. For example, how many cases occurred in 2019? How many occurred in the last ten years? In whom? Once we gather this information then we can compare what we are seeing now with the normal patterns.
- Second, we need to conduct risk studies where we compare the risk of the condition in vaccinated people with the risk in unvaccinated people. There are a number of scientific methods to do this. If there is no difference then we might conclude that the vaccine is unlikely to be causing the problem, alternatively, if there is a greater risk in the vaccinated people then we might conclude that the vaccine is causing some of these events.
What do we do if the vaccine is to blame?
If the risk is as small, as it currently appears to be, then we need to ask ourselves if it is worth using these vaccines and if so, in whom. In a country with no COVID-19 there is no risk of blood clots from natural COVID-19 infection. If there is a vaccine that does not carry this risk (so far this risk is not associated with the Pfizer or Moderna vaccines) then it may be a better choice. However, in a setting where there is COVID-19, or no alternative vaccine available, then the AZ and Janssen vaccines will save many, many lives and also dampen the risk of dangerous variants developing. While these vaccines are halted because of a 1-4 in a million risk of blood clots (and <1 per million death) many thousands have lost their lives due to COVID-19 and the speed at which we might otherwise control this plague is slowed.
References:
[i] https://www.medsafe.govt.nz/consumers/leaflets/oralcontraceptives.asp
[ii] https://www.weather.gov/safety/lightning-odds
[iii] https://www.weather.gov/safety/lightning-odds
Helen Petousis-Harris is an Associate Professor in the Department of General Practice and Primary Health Care at the University of Auckland. She is also the Director of the Vaccine Datalink and Research Group.
For more information on COVID-19, head to the Ministry of Health website.
Disclaimer: The ideas expressed in this article reflect the author’s views and not necessarily the views of The Big Q.
You might also like:
Q+A: Will a possible new COVID vaccine mean the end of the pandemic?
Corruption and the COVID-19 vaccine: The looming problem of distribution?
