
By Helen Petousis-Harris
How serious is the new coronavirus pandemic? Are we set for a global pandemic? Helen Petousis-Harris investigates.
Just over a month ago the emergence of a previously unseen disease-causing virus was announced. It is officially called 2019 novel coronavirus, or 2019nCoV for short and it is now reasonably established that the virus is transmitted from person to person and most typically causes fever and cough. This is not an exceptional event per se, after all, infectious diseases have to come from somewhere. Every infection known to man began as a novel new thing at one point. What is new is the fact we have the technology to identify it fast, track it, stop it, cure it, and vaccinate against it. Now we can literally watch the birth of a new human infection in real time. Never before has there been so much true, and false, information exploding through our media channels, of which there are vast numbers, reaching almost every community on earth.
Emergence of new infectious diseases
When a new disease emerges, there are two stages. First is the introduction of the new infection into the population (in this case some unsuspecting humans). This usually involves the jump from animal to human, called zoonosis and it happens quite a lot. The second stage is the establishment of the infection in humans and sustained person-to-person transmission. Often this occurs when an infection in animals mutates in a way that helps it infect a human and then further mutations might occur that enable it to successfully jump between people.
A really good recent example of an animal infection jumping into humans then becoming a common human disease is the 2009 Swine Flu. This virus jumped from pigs and caused a global pandemic. Eleven years later this strain of influenza is just one of the many strains of flu that we still see every year. Just a couple of years after it emerged most people in New Zealand had been infected, though not all of them got sick.
How Infectious?
This is one of the most important questions, and one there is as yet no clear answer to. In order to accurately estimate infectiousness (aka basic reproduction number) we need to know how many people have been infected and who they got it from. Since quick testing became widely available (in the last couple of weeks) more and more people can be diagnosed. Epidemiologists are able to model the transmission of the infection and estimate how many people might actually have it but are not sick enough to visit a hospital, or even have no symptoms at all. There are probably lots of mild cases that are not being tested. Modelling from the Imperial College in London has estimated around 100,000 (30,000 – 200,000) are likely to be infected. Of course, the more you test the more you are likely to find.
Several research groups have provided estimates of the infectiousness of this virus and they generally land in the vicinity of one infectious person infecting 2-3 other people. That is a little bit more than your average influenza (about 1.4 – 4), way less infectious than measles (12-18), whooping cough (12-17), chickenpox (8-10), and many other infections. It is not yet established whether or not the infection can be spread by a person who has no symptoms but this is a question of burning importance. Infections like flu and the common cold can be spread by people who have no symptoms. In these cases, the viruses are carried into the air when they breathe and speak.
Finally, one phenomenon that can throw off the estimates is that of the super spreader. Super spreaders played an important role in the transmission of SARS (a related coronavirus that caused around 800 deaths earlier this century). Say the average infected person passes the virus on to 2 or 3 others, a super spreader might pass it on to at least 6, or more – just a wild card that can further complicate things.
How Deadly?
To answer this question, we really need to know how many people have actually been infected. If we only include notifications then around 2-3% notified die. If far more have been infected then this will be much lower. Worst case scenario, this is still much less deadly than many infectious diseases we see every day and possibly more akin to seasonal influenza. Time will tell.
Remember the 2009 swine flu pandemic? At first people thought the death rate was 10%, but after more information became available it became apparent that it was only 0.1%, or 1% of the earlier estimates. This is in line with regular influenza.
Those most severely affected tend to be older and frailer than the general population. In a study that reported on the first 99 cases hospitalised in Wuhan, the average age was 55-years, 67 were men, and half had underlying chronic diseases. There were no children in this group, the youngest was 21 and 90% were over 40.
Just to put this in perspective, each year there are an estimated 84,000 – 92,000 influenza-related deaths in China.
Of course, how deadly also depends on the health systems available. The recent measles epidemics in NZ and Samoa illustrated this grim reality very clearly. No one in NZ died thanks to fancy modern medicine (although there were some close calls). However, we exported it to our Pacific neighbours, in particular Samoa, where over 80 young people died. The consequences of this coronavirus getting loose in countries with poorly developed health systems is frightening and something we must all do our part in helping to prevent.
Current situation
As of writing (which will be at least a bit out of date when you read this) this was the situation.
- 14,557 notified cases of which 14,411 (99%) have been in China. Of these around 15% are severely ill.
- China is moving heaven and earth to contain this within its borders
- No new cases outside China were reported over Saturday/Sunday. The first death outside China was reported and occurred in the Philippines
- A serious misinfodemic is occurring – fake news, unsubstantiated rumours, and crazy talk are spreading way more than the coronavirus. This is concerning and the World Health Organisation (WHO) have all hands to the deck to try to counter the nonsense.
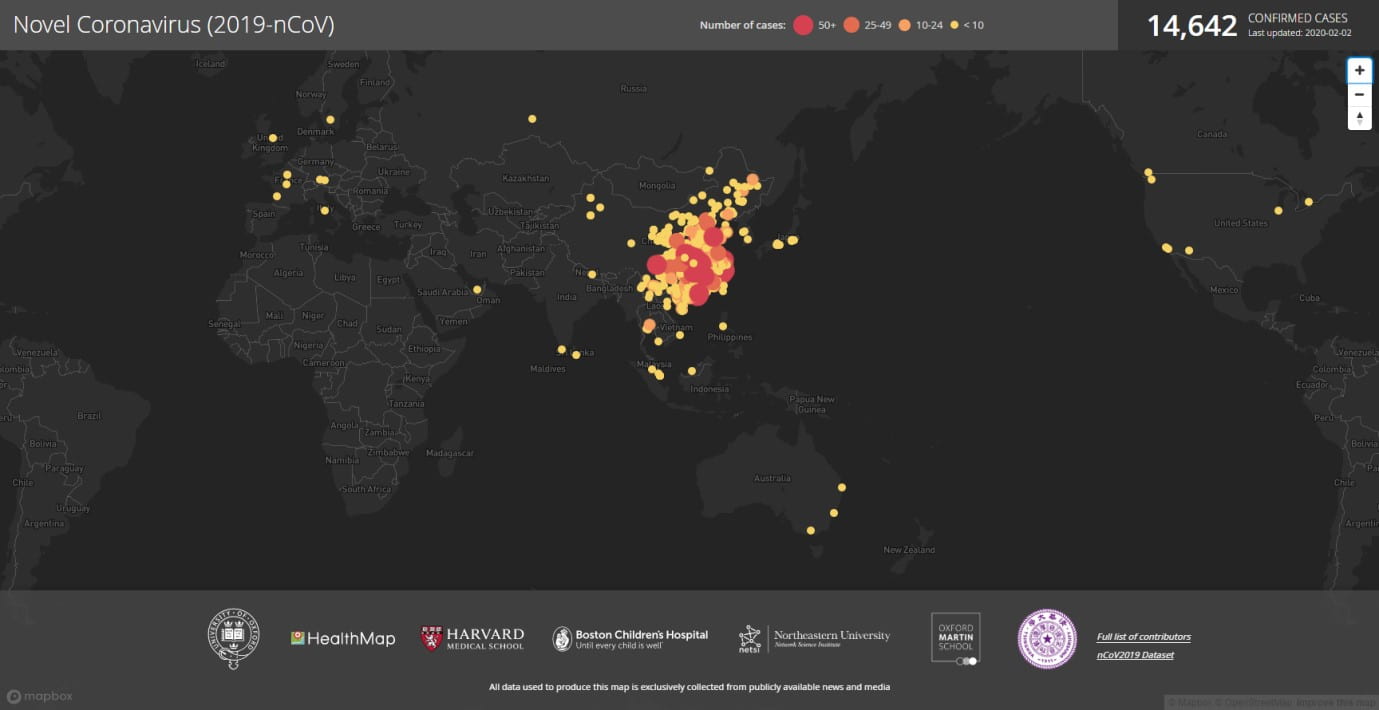
Figure 1. Click Here for an updated interactive map
Can it be controlled?
Maybe. Based on work at the Imperial College in London, in order to control this outbreak interventions will need to block at least 60% of transmissions. Because there are not yet any medicines or vaccines control relies purely on quick detection and isolation of people who have symptoms. Again, much depends on the ability of people with little or no symptoms to transmit this infection, and we do not really know the answer to this yet.
The effort to contain this infection in the province (Hubei) where most cases are is unprecedented. Never before we have seen such intensive control measures. It remains to be seen if this will work.
Will there be a cure?
Probably. The WHO along with laboratories and governments all over the world are working on treatments for this infection and regulatory agencies such as the US Federal Drug Administration are leveraging the vast FDA experience to facilitate the development of potential therapies. There are a range of approaches for effective drugs and the bonus is that there are several already in the pipeline for other infections that could be easily adapted for this coronavirus.
Will there be a vaccine?
Yes, if this thing does not go away. The technology is there, several approaches are likely to yield an effective vaccine, from nanoparticle, viral vector, subunit adjuvanted, live attenuated… These are all established technologies for vaccine development, and like potential therapeutics there are examples in the pipeline for other infections including coronaviruses such as SARS and MERS, it is really just a matter of switching the target (in this case the 2019nCoV spike protein). Numerous laboratories and pharmaceutical companies have shifted resource and focus onto a 2019 coronavirus vaccine. However, vaccines must undergo more extensive testing than other medicinal products as they are usually used in healthy rather than sick people. Best guess is at least a year, but if we can’t get this infection back in its box then vaccines will be the ideal long-term solution.
We also have a misinfodemic
The unprecedented flow of information has enabled remarkable progress to be made in both controlling this outbreak as well as potential cures and vaccines, all in a month. However, along with useful facts have come rumours, and misinformation. This has led to confusion, politicking, stigmatisation, hysteria, and worst of all, xenophobia. The WHO are extremely concerned and are pouring efforts into addressing the misinformation. However, they can’t do it alone. This is a problem that requires effort at all levels – from government, to health sector, to communities and key influencers. While not all of us can find a cure or invent a vaccine, we can be part of the solution to the misinfodemic and not part of the problem by fact checking before sharing, and sharing good information from a reputable source. Try Snopes or some other fact-checking website.
Finally – risk communication
Risk communication in a vital part of any crisis and while this may seem obvious it is often overlooked by those responsible for coordinating it. Risk communication is an interactive process whereby information that helps people understand their risk is exchanged. It helps protect people’s health during the crisis. If the key messages do not reach everyone then people will lose trust in the leaders who are there to protect them, which is why all stakeholders should be involved – in a coordinated team effort. Also, there are economic impacts that occur when panic occurs. The public should expect regular proactive communications from their Governments and Health Ministries, even when there are lots of things not yet known. They should be told what is being done and why. These messages should not only come from the officials in government but through a variety of expert sources, as well as through the community. For example, church leaders, local doctors, and other trusted people in the community.
Also, many people don’t watch TV anymore or listen to the radio. They have Netflix and Spotify. News and information come through Facebook, Twitter, YouTube, WeChat, and so on. So, no matter how textbook perfect the official communication on TV news is, many people will either not have seen it, not understand it, or have no trust in the messenger. Social media feed is tailored to the individual’s interests so messages need to be targeted to the local community.
Through effective risk communication people in NZ will understand that right now there is almost zero chance of them contracting the 2019nCoV, face masks are of little value, most people do not die, in fact it is likely most people do not even get very sick, influenza kills about 400,000 people in the world each year, and that the global response is unprecedented and based on the best information available as it comes to hand.
Helen Petousis-Harris is an Associate Professor in General Practice and Primary Healthcare at the University of Auckland. She is an expert in vaccines and vaccination.
For more information on COVID-19, head to the Ministry of Health website.
Disclaimer: The ideas expressed in this article reflect the author’s views and not necessarily the views of The Big Q.
You might also like:
